By Rustam Iuldashov
30 years lived experience with chronic migraine | Sources: 25 peer-reviewed references including Frontiers in Neurology (n=356,441), Communications Biology (CGRP-anxiety mechanism), JAMA Neurology (UNITE RCT, n=237) | Last updated: March 11, 2026
Medical Review: This content is based on peer-reviewed research from Frontiers in Neurology, Current Pain and Headache Reports, Communications Biology, Physiological Reviews, JAMA Neurology, Neurology and Therapy, Heliyon, Journal of Clinical Medicine, Headache, and the Handbook of Clinical Neurology.
Important Notice: This article is for informational purposes only and does not replace professional medical advice. The author is not a licensed physician or healthcare professional. Always consult your doctor before making changes to your treatment plan.
Key Takeaways
- Migraine and anxiety share a bidirectional relationship: each condition increases the risk of developing the other[1][4]
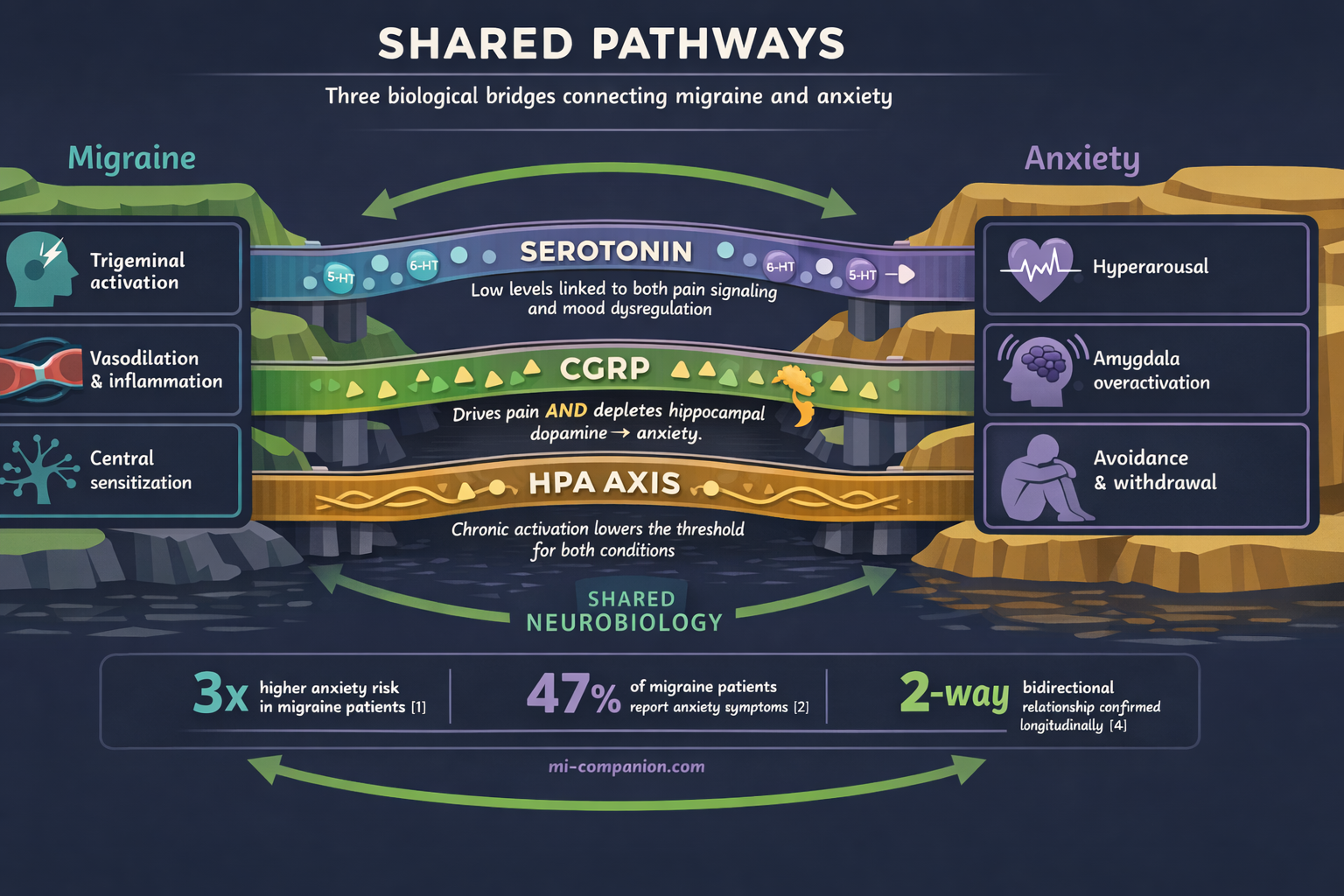
- They share fundamental neurobiology — serotonin dysfunction, CGRP activity in the amygdala and hippocampus, and HPA axis dysregulation[5][6][13]
- CGRP, the molecule central to migraine pain, directly causes anxiety by depleting dopamine in the hippocampus[8]
- The body “remembers” repeated attacks as trauma, keeping the nervous system in a state of chronic hypervigilance that feeds both conditions[13]
- Interictal burden — the anticipatory anxiety between attacks — may drive more disability than the attacks themselves[9][10]
- CGRP-targeted treatments can improve both migraine and anxiety symptoms simultaneously, and CBT directly dismantles the fear-avoidance cycle[14][17]
- Treating only one condition while ignoring the other leaves the loop intact. The most effective approach addresses both[19]
You’re lying in bed on a Sunday night. No headache. No aura. But your chest is tight. Your mind is already scanning tomorrow’s calendar — the fluorescent lights, the deadlines, the chance that it will come. You haven’t had a migraine in five days, but your brain is already bracing for the next one.
This is what chronic migraine does. It doesn’t just steal the days when pain arrives. It colonizes the days in between.
If this feeling sounds familiar, you’re not imagining things. And you’re far from alone.
Migraine and anxiety are two of the most common neurological and psychiatric conditions on earth. But they don’t simply coexist. They feed each other in a loop so tight that treating one without addressing the other often means treating neither. The neuroscience behind this loop reveals something genuinely surprising — and practically useful — about how your brain works.
The Numbers That Stopped Me Cold
A meta-analysis of over 15,000 people with migraine and 77,000 controls found that people with migraine are three times more likely to experience anxiety — an odds ratio of 3.18.[1] That’s not a subtle association. That’s a red flag in neon.
It goes deeper. Anxiety symptoms appear in up to 47% of people living with migraine.[2] A population-based study of over 356,000 migraine patients found anxiety prevalence of 24.6%, compared to 14.1% in matched controls — a twofold increased risk.[3]
3× higher anxiety risk in migraine patients (OR = 3.18, n=15,133 vs 77,453 controls)[1]
47% of migraine patients report anxiety symptoms[2]
24.6% vs 14.1% — anxiety prevalence in migraine patients vs matched controls (n=356,441)[3]
But here’s the part that reframes everything: the relationship runs in both directions. Longitudinal research by Breslau and colleagues demonstrated that migraine increases the risk of developing anxiety, and anxiety increases the risk of developing migraine.[4] Each condition predicts the future onset of the other. This isn’t correlation. This is a feedback loop hardwired into your neurobiology.
Same Wiring, Different Symptoms
Why would a headache disorder and a mood disorder be so tangled? Because they share the same neural infrastructure.
Serotonin — the molecule that does too much. During a migraine attack, serotonin levels drop.[5] This depletion leaves blood vessels without their normal tone and fires up the trigeminal pain pathway. The same serotonin system that derails during migraine is the one regulating mood, sleep, and anxiety. Genetic variations in the enzyme that produces serotonin — tryptophan hydroxylase — have been linked to increased susceptibility to both conditions.[5] One factory. Two assembly lines. Both malfunctioning.
CGRP — the migraine molecule that also drives fear. Calcitonin gene-related peptide has become the star of migraine research. When the trigeminal nerve fires during an attack, it floods surrounding blood vessels with CGRP, triggering inflammation and pain.[6] But CGRP doesn’t stay in pain circuits. It concentrates heavily in the amygdala — the brain’s threat-detection center — and in the hippocampus, where memories and emotional regulation live.[7]
A 2024 study showed that CGRP directly causes anxiety by depleting dopamine in the hippocampus. The same molecule that gives you migraine pain literally rewires your emotional thermostat toward anxiety.
Here’s the finding that changed how I understand my own brain: a 2024 study in Communications Biology showed that CGRP directly causes anxiety by depleting dopamine in the hippocampus.[8] The mechanism is elegant and unsettling. CGRP activates an enzyme called MAOB that breaks down dopamine — the neurotransmitter your brain needs to stay calm and focused. The same molecule that gives you migraine pain literally rewires your emotional thermostat toward anxiety.
The amygdala connection. CGRP signaling between the parabrachial nucleus and the central nucleus of the amygdala drives fear and anxiety responses through sensitization of NMDA receptors — the same glutamate receptors involved in central sensitization during migraine.[6] Think of it as your brain’s alarm system stuck on high sensitivity. Every signal gets amplified, whether it’s pain or worry.
The Body Remembers What the Mind Tries to Forget
Bessel van der Kolk writes in The Body Keeps the Score that trauma and chronic stress don’t just live in our thoughts — they become embedded in our bodies. The nervous system doesn’t forget. It adapts, often in ways that create new problems.
This insight is profoundly relevant to migraine. Each attack is a neurological event, yes. But it is also a somatic experience that your body records. The nausea, the light sensitivity, the helplessness of lying in a dark room — these aren’t abstract memories. They become encoded in your nervous system’s threat library. Over time, your brain doesn’t need an actual trigger. The anticipation of an attack becomes sufficient to activate the same stress pathways.
Van der Kolk’s work explains why chronic pain conditions so often travel with anxiety: the body stays in a state of defensive readiness long after the immediate threat has passed. Your muscles tense before you consciously feel afraid. Your breathing shallows. Your heart rate creeps up. The migraine hasn’t started, but your body is already responding as if it has.
This is the physiological basis of what researchers call allostatic load — the cumulative cost of chronic stress on a system designed for acute emergencies.[13] Your hypothalamic-pituitary-adrenal (HPA) axis, the body’s central stress command, runs chronically hot. Ordinary stimuli start registering as threats. A flickering light. A strong smell. A tight deadline. Each one becomes a potential trigger — not because you’re fragile, but because your nervous system has been trained by years of repeated neurological assault.
This hypervigilance isn’t a character flaw. It’s a biological adaptation to living with a brain that can ambush you without warning.
The Invisible Suffering Between Attacks
There’s a concept in headache medicine that deserves far more attention: interictal burden — the suffering that happens when you don’t have a migraine.
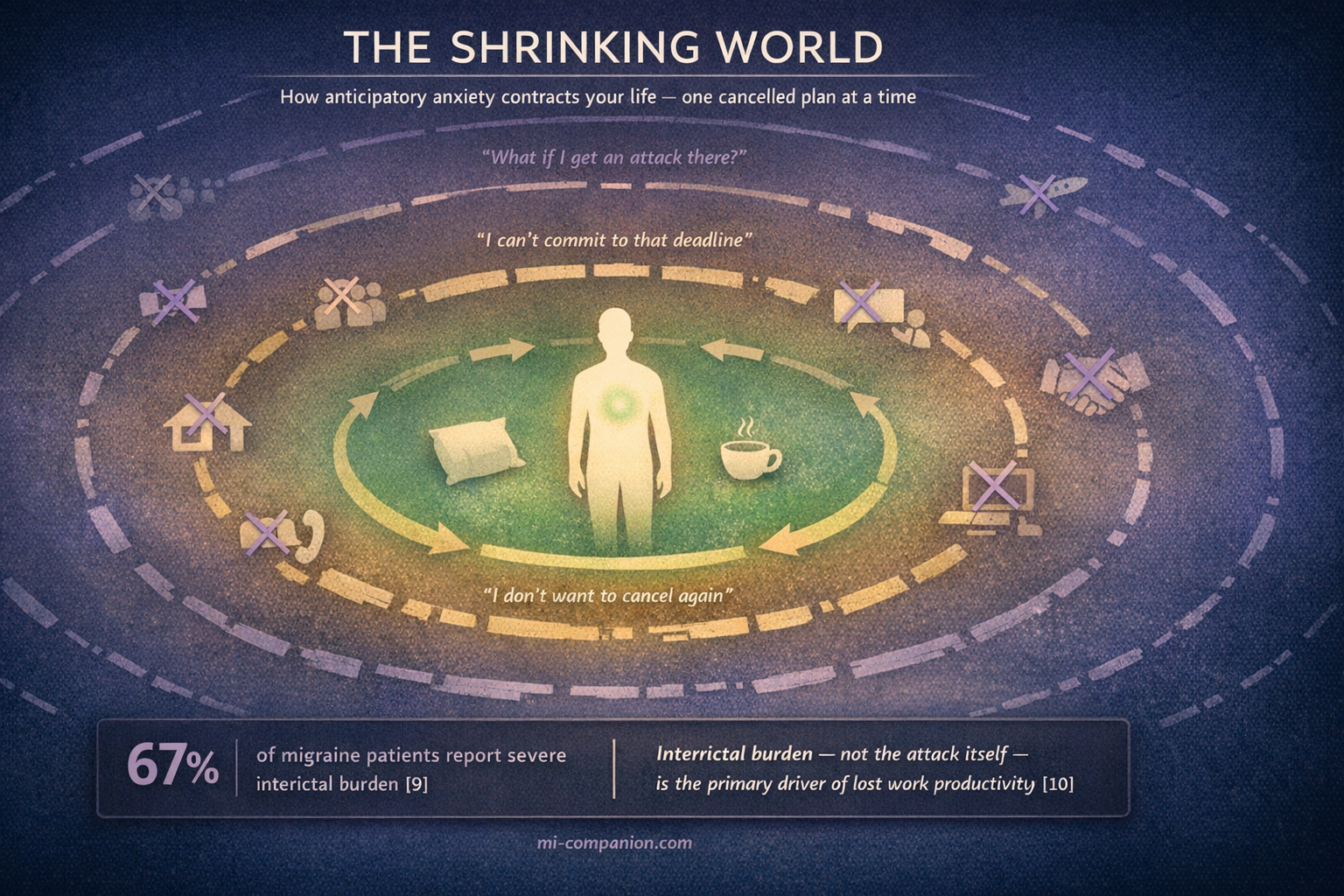
Most research and treatment focuses on the attack itself. But growing evidence shows that the time between attacks can inflict equal damage. In a survey of people with migraine, 67% reported severe interictal burden.[9] A 2026 Japanese study found something remarkable: interictal burden — not the headache itself — was the primary driver of work productivity loss.[10]
What does interictal burden look like? Anticipatory anxiety. Fear of the next attack. Avoidance of anything that might provoke one. Difficulty making plans or commitments. Researchers have coined a term for this: cephalalgiaphobia — the fear of headache itself.[11]
This creates a textbook fear-avoidance cycle. You fear the next attack, so you skip the dinner, cancel the trip, say no to the project. The avoidance shrinks your world. The smaller world increases stress and isolation. The stress lowers your migraine threshold. The attack comes sooner. The fear deepens.
Guy Winch describes this pattern in Emotional First Aid: chronic illness creates what he calls “psychological wounds” — not just the disease itself, but the secondary losses it inflicts. Loss of control. Loss of predictability. Loss of the identity you had before the condition took over. These wounds, left untreated, fester. The person who once traveled freely now declines invitations. The professional who thrived under pressure now catastrophizes about deadlines. The friend who was always available now isolates — not because of pain, but because of the fear of pain that hasn’t arrived yet.
I’ve lived inside this cycle for 30 years. There were stretches when I managed migraine and anxiety simultaneously without realizing they were the same problem wearing different masks.
⚠️ When to Seek Emergency Help
If you experience sudden, severe anxiety with chest pain, difficulty breathing, or feelings of impending doom alongside a new or unusual headache pattern, seek immediate medical evaluation. Sudden panic symptoms combined with the worst headache of your life could signal a serious neurological event.
Call your local emergency number immediately. Do not use this article to self-diagnose.
Breaking the Loop: What Actually Works
Because migraine and anxiety share biological pathways, treating one often helps the other. But the approach matters.
CGRP-targeted treatments. The new generation of migraine-specific preventives — monoclonal antibodies like erenumab, galcanezumab, and fremanezumab — don’t just reduce migraine days. A 2024 review found that erenumab and galcanezumab were associated with significant improvements in concurrent anxiety and depression.[14] In a real-world Greek registry, 43% of chronic migraine patients with psychiatric comorbidities saw their anxiety severity decrease or resolve entirely after fremanezumab treatment.[15] The 2025 UNITE trial — the first randomized controlled trial specifically designed to study a CGRP antibody in patients with comorbid migraine and major depressive disorder — showed fremanezumab significantly reduced both migraine days and depressive symptoms.[16]
43% of chronic migraine patients with psychiatric comorbidities saw anxiety resolve or decrease with CGRP treatment[15]
UNITE trial — first RCT showing CGRP antibody improves both migraine and major depression (n=237)[16]
The biological logic is straightforward. If CGRP drives both pain and anxiety through shared pathways, blocking CGRP should quiet both.
Cognitive behavioral therapy. A 2025 systematic review and meta-analysis of 50 randomized trials (over 6,000 adults) found that CBT, relaxation training, and mindfulness-based therapies each reduce migraine frequency.[17] But CBT does something medications cannot: it directly targets the anticipatory anxiety and avoidance behaviors that drive interictal burden.
CBT for migraine works by identifying the thought patterns that amplify the fear cycle — catastrophizing about attacks, overestimating triggers, avoiding life out of proportion to actual risk.[18] A three-armed RCT found that migraine-specific CBT led to a 30% or greater reduction in headache days for 44% of participants at 12-month follow-up.[18] When combined with preventive medication, it addresses both the neurological and psychological architecture of the loop.
The dual approach. The emerging clinical consensus is clear: for people with comorbid migraine and anxiety, treating only one condition leaves the other to keep stoking the fire.[19] Headache specialists are increasingly urged to screen routinely for anxiety, and mental health professionals need to understand that their anxious patients may have an untreated neurological component.[2]
Rewriting the Story of Your Brain
Susan Cain, in Bittersweet, makes an observation that resonates deeply with anyone living at the intersection of chronic pain and chronic worry: the most profound growth often comes not from escaping suffering, but from integrating it. She writes about the power of acknowledging vulnerability — of allowing sadness and limitation to coexist with meaning and purpose.
For those of us with migraine, this isn’t abstract philosophy. It’s a daily practice. The question isn’t whether your brain will sometimes betray you with pain and anxiety. It will. The question is what you build around that reality.
Understanding the bidirectional link gives you something powerful: an explanation. Your anxiety isn’t a personal weakness. Your migraine isn’t “just a headache.” They are two expressions of a shared neurological vulnerability — and that vulnerability responds to treatment.
Ask your doctor about screening. If you have migraine, request anxiety screening with the GAD-7 — it takes two minutes. If you have anxiety, mention your headache patterns, even if they seem unrelated.[2]
Track what happens between attacks. Don’t just log pain days. Note your worry levels, avoidance behaviors, difficulty planning. This data helps your clinician see the full picture — and it helps you see the pattern.
Consider combination treatment. The most effective approach for comorbid migraine and anxiety often pairs a migraine-specific preventive with behavioral therapy.[19] Neither alone is enough when both conditions are active.
Break the avoidance cycle — gently. Accept one invitation you’d normally decline. Make one plan without a backup excuse. Each time you engage with life despite the fear of an attack, you weaken the neural pathway that says “danger.” Van der Kolk’s research shows that the body can be retrained — slowly, safely, through repeated exposure to the experiences it has learned to fear.
The migraine-anxiety loop is real. It’s biological. And it can be broken — not by fighting your brain, but by understanding it.
⚕️ Important Medical Disclaimer
This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. The author, Rustam Iuldashov, is not a licensed physician, neurologist, or healthcare professional. He is a patient advocate with 30 years of personal experience living with chronic migraine.
All clinical claims in this article are sourced from peer-reviewed research published in indexed medical journals. Study designs and sample sizes are noted where applicable.
Always consult a qualified healthcare provider for questions about your individual health, migraine treatment, medication decisions, or mental health concerns. Do not adjust, start, or stop any medication — including anti-anxiety medications or migraine preventives — based on this article alone.
This content was last reviewed for accuracy on March 11, 2026.
References
- Karimi L, Wijeratne T, Crewther SG, Evans AE, Afshari L, Khalil H. “Migraine: A Review on Its History, Global Epidemiology, Risk Factors, and Comorbidities.” Frontiers in Neurology, 13:800605 (2022). doi:10.3389/fneur.2022.800605. Study design: Systematic review / Meta-analysis. n=15,133 migraine patients, 77,453 controls.
- Seng EK, Buse DC, et al. “Anxiety Disorders, Anxious Symptomology and Related Behaviors Associated With Migraine: A Narrative Review of Prevalence and Impact.” Current Pain and Headache Reports, 29:21 (2025). doi:10.1007/s11916-024-01312-9. Study design: Narrative review.
- Engel H, Gal A, Engel T, et al. “Migraine Epidemiology, Comorbidities and Therapeutic Landscape: A National Population-Based Study.” Frontiers in Neurology, 17:1743203 (2026). doi:10.3389/fneur.2026.1743203. Study design: Population-based cohort. n=356,441 migraine patients, 4,257,890 controls.
- Breslau N, Davis GC, Andreski P. “Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of young adults.” Psychiatry Research, 37(1):11–23 (1991). doi:10.1016/0165-1781(91)90102-u. Study design: Prospective cohort. n=1,007.
- Deen M, Correnti E, Bhatt DK, et al. “Serotonin and CGRP in Migraine.” Annals of Neurosciences, 21(2):70–72 (2014). doi:10.5214/ans.0972.7531.210209. Study design: Review.
- Russo AF. “Calcitonin Gene-Related Peptide (CGRP): A New Target for Migraine.” Annual Review of Pharmacology and Toxicology, 55:533–552 (2015). doi:10.1146/annurev-pharmtox-010814-124701. Study design: Review.
- Hay DL, Garelja ML, Poyner DR, Walker CS. “CGRP physiology, pharmacology, and therapeutic targets: migraine and beyond.” Physiological Reviews, 103(2):1565–1644 (2023). doi:10.1152/physrev.00059.2021. Study design: Comprehensive review.
- Hong Y, Kim J, Park J, et al. “CGRP causes anxiety via HP1γ–KLF11–MAOB pathway and dopamine in the dorsal hippocampus.” Communications Biology, 7:351 (2024). doi:10.1038/s42003-024-05937-9. Study design: Preclinical (animal model).
- Buse DC, et al. “Interictal Burden of Migraine: A Narrative Review.” Headache Practice & Research (2025). Study design: Narrative review. Survey: n=506.
- Suzuki N, et al. “Interictal burden, not ictal burden, drives work productivity impairment in headache disorders.” The Journal of Headache and Pain, 27:29 (2026). doi:10.1186/s10194-026-02284-4. Study design: Cross-sectional.
- Rogers DG, Protti TA, Smitherman TA. “Fear, Avoidance, and Disability in Headache Disorders.” Current Pain and Headache Reports, 24(7):33 (2020). doi:10.1007/s11916-020-00865-9. Study design: Review.
- Argyriou AA, et al. “Effects of Fremanezumab on Psychiatric Comorbidities in Difficult-to-Treat Patients with Chronic Migraine.” Journal of Clinical Medicine, 12:4526 (2023). doi:10.3390/jcm12134526. Study design: Prospective registry. n=107.
- Pellesi L, et al. “Hypervigilance, Allostatic Load, and Migraine Prevention.” Neurology and Therapy, 10:469–484 (2021). doi:10.1007/s40120-021-00250-7. Study design: Review.
- Elkholy SH, et al. “Improvement of comorbid anxiety and depression in patients with migraine treated with injectable preventive CGRP antagonists.” Heliyon, 10(4):e25698 (2024). doi:10.1016/j.heliyon.2024.e25698. Study design: Systematic review of clinical evidence.
- Argyriou AA, et al. “Effects of Fremanezumab on Psychiatric Comorbidities in Difficult-to-Treat CM Patients.” Journal of Clinical Medicine, 12:4526 (2023). doi:10.3390/jcm12134526. Study design: Prospective registry post hoc. n=107 (65 with psychiatric comorbidities).
- Lipton RB, et al. “Fremanezumab for the Treatment of Patients With Migraine and Comorbid Major Depressive Disorder: The UNITE Randomized Clinical Trial.” JAMA Neurology (2025). doi:10.1001/jamaneurol.2025.1234. Study design: RCT. n=237.
- Minen MT, et al. “Behavioral interventions for migraine prevention: A systematic review and meta-analysis.” Headache, 65(2) (2025). doi:10.1111/head.14885. Study design: Systematic review / Meta-analysis. n=6,024.
- Klan T, Gaul C, et al. “Efficacy of Cognitive-Behavioral Therapy for the Prophylaxis of Migraine in Adults: A Three-Armed Randomized Controlled Trial.” Frontiers in Neurology, 13:852616 (2022). doi:10.3389/fneur.2022.852616. Study design: RCT. n=128.
- Smitherman TA, et al. “Psychiatric comorbidities of migraine.” Handbook of Clinical Neurology, 199:43–50 (2024). doi:10.1016/B978-0-12-823357-3.00013-6. Study design: Review chapter.
- Duan S, Ren Z, et al. “Associations between anxiety, depression with migraine, and migraine-related burdens.” Frontiers in Neurology, 14:1090878 (2023). doi:10.3389/fneur.2023.1090878. Study design: Cross-sectional.
- Bae JY, Kim NY. “Cognitive Behavioral Therapy for Migraine Headache: A Systematic Review and Meta-Analysis.” Medicina, 58(1):44 (2022). doi:10.3390/medicina58010044. Study design: Systematic review / Meta-analysis. n=621.
- Karimi L, Crewther SG, Wijeratne T, et al. “The Migraine-Anxiety Comorbidity Among Migraineurs: A Systematic Review.” Frontiers in Neurology, 11:569405 (2020). doi:10.3389/fneur.2020.569405. Study design: Systematic review. n=8 studies.
- Lampl C, Seng E, Vincent M, et al. “Interictal burden in migraine patients at the outset of CGRP monoclonal antibody prevention.” The Journal of Headache and Pain, 25:220 (2024). doi:10.1186/s10194-024-01927-8. Study design: Cross-sectional survey. n=500.
- Cuciureanu DI, et al. “Migraine Comorbidities.” Life, 14(1):74 (2024). doi:10.3390/life14010074. Study design: Review.
- Shapiro RE, Nicholson RA, Seng EK, et al. “Migraine-Related Stigma and Its Relationship to Disability, Interictal Burden, and Quality of Life: Results of the OVERCOME (US) Study.” Neurology, 102(3):e208074 (2024). doi:10.1212/WNL.0000000000208074. Study design: Population-based cross-sectional. n=59,001.

How We Create Content
- Peer-reviewed sources only. Frontiers in Neurology, Current Pain and Headache Reports, Communications Biology, Physiological Reviews, JAMA Neurology, Neurology and Therapy, Heliyon, Journal of Clinical Medicine, Headache, Handbook of Clinical Neurology, The Journal of Headache and Pain, Neurology, Life, Medicina, Psychiatry Research, Annals of Neurosciences, Annual Review of Pharmacology and Toxicology.
- Study transparency. Study design and sample sizes noted for all clinical references.
- Source verification. All claims backed by numbered references with DOI links.
- Experience + Science. 30 years personal migraine experience combined with peer-reviewed evidence.
- Regular updates. Articles reviewed when significant new research emerges.
- No conflicts of interest. No funding from pharmaceutical companies, psychiatric medication manufacturers, or mental health service providers.
Track Both Sides of the Loop
Migraine Companion helps you log attacks, triggers, mood, and anxiety levels together — so you and your doctor can see the full picture of how migraine and mental health interact in your life.
Last reviewed: March 2026
Next scheduled review: September 2026