
By Rustam Iuldashov
30 years lived experience with chronic migraine | Sources: 24 peer-reviewed references including Cephalalgia, Neurology, Frontiers in Neurology, Frontiers in Human Neuroscience, Psychophysiology, Scientific Reports | Last updated: March 9, 2026
Medical Review: This content is based on peer-reviewed research from Cephalalgia, Neurology, Frontiers in Neurology, Frontiers in Human Neuroscience, Frontiers in Public Health, Psychophysiology, Scientific Reports, Molecular Medicine, and International Journal of Yoga.
Important Notice: This article is for informational purposes only and does not replace professional medical advice. The author is not a licensed physician or healthcare professional. Always consult your doctor before making changes to your treatment plan.
Key Takeaways
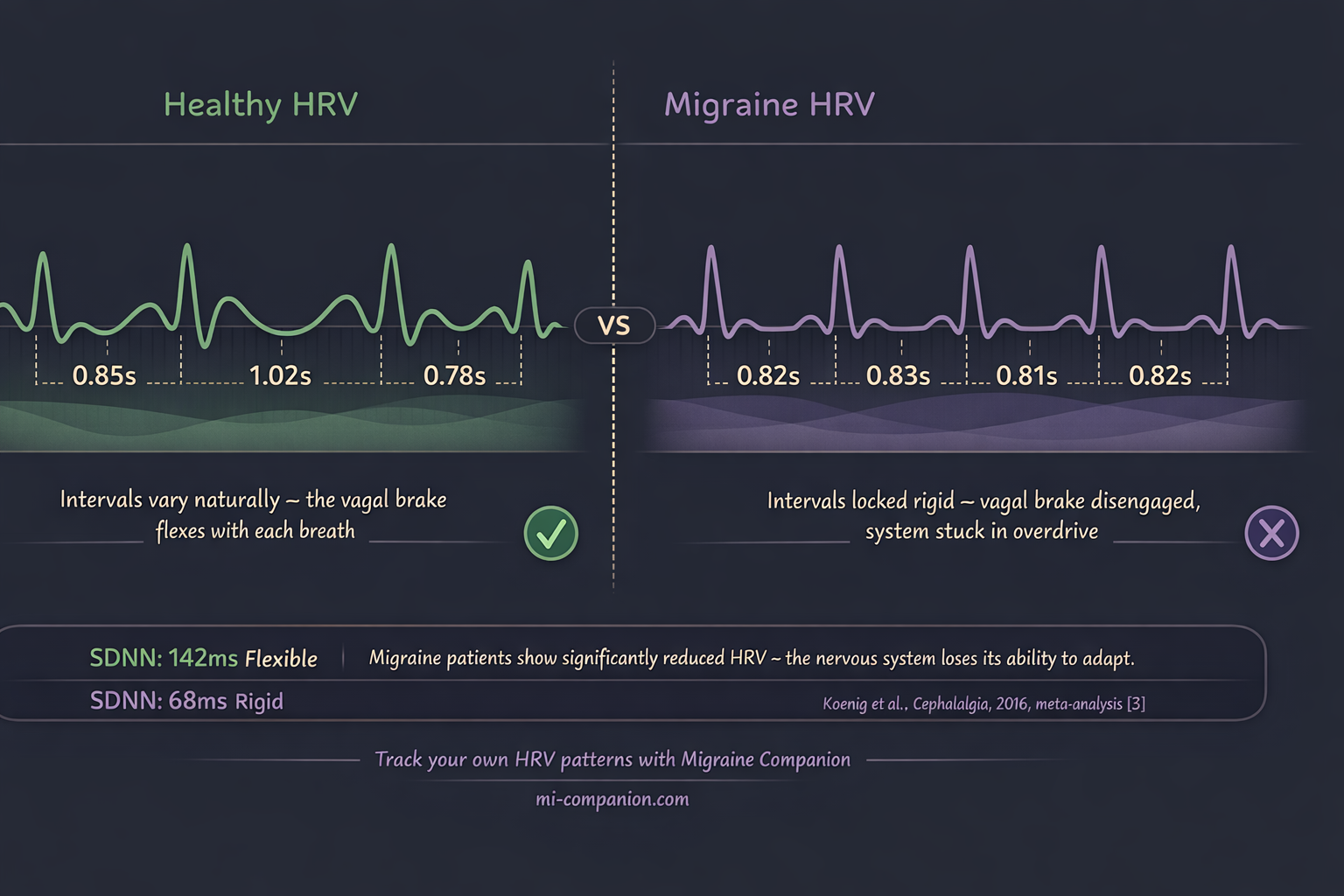
- Migraine brains show reduced vagal tone and lower heart rate variability — the parasympathetic brake is weakened[3, 4]
- Vagus nerve activation suppresses cortical spreading depression by up to 40%, reduces glutamate in pain pathways, and dials down neurogenic inflammation through the cholinergic anti-inflammatory pathway[7, 8, 9]
- FDA-cleared vagus nerve stimulation devices show meaningful clinical benefit for migraine but cost ~$700/month[11, 12, 14]
- Three free techniques activate the same nerve: slow breathing at ~6 breaths/minute, cold water on the face (dive reflex), and humming (vibratory stimulation)[15, 20, 24]
- Consistency matters: daily practice improves baseline vagal tone over weeks — think physical therapy for the nervous system[17]
- These techniques complement, never replace, medical treatment. Work with your healthcare provider.
Cold water on the wrist. A slow exhale. A hum that vibrates in your chest.
These aren’t wellness trends. They’re vagus nerve activators — and for people who live with migraine, they may be the simplest, most underused tools science has validated.
The vagus nerve is the longest cranial nerve in your body. It wanders from brainstem to gut, threading through your neck, heart, and lungs — a two-lane highway between brain and body.[1] Its Latin name means “wanderer.” That wandering is exactly what makes it powerful. When the vagus nerve fires, your entire nervous system shifts — from fight-or-flight to rest-and-recover.[2]
For migraine, that shift changes everything, especially when dealing with the hyperexcitable brain that characterizes the condition.
Your Migraine Brain Has a Vagal Problem
Most people think of migraine as a headache. It isn’t. It’s a nervous system disorder — and the vagus nerve sits at the control panel.
A 2016 meta-analysis in Cephalalgia pooled data from multiple studies and found something striking: people with migraine have significantly lower vagally mediated heart rate variability than healthy controls.[3] Translation: the nerve responsible for calming your system down is underperforming. A cross-sectional study confirmed this pattern, showing parasympathetic dysfunction dominated during attacks — and that HRV dropped further as pain climbed.[4] The worse the migraine, the weaker the brake.
Here’s where it gets clinically relevant. A study of chronic migraine patients found that those whose vagal function was still intact responded dramatically better to preventive medication — gaining nearly 3.5 more headache-free days per month than patients with impaired vagal tone.[5] Other researchers have documented the same autonomic imbalance: reduced parasympathetic activity, sympathetic predominance, especially in migraine with aura.
Picture a car with the accelerator jammed and the brake pedal soft. That’s the migraine nervous system. The sympathetic gas pedal is floored. The vagal brake barely engages.[3, 6]
The encouraging part? You can strengthen that brake.
How Vagal Activation Fights Migraine — The Biology
Before the techniques, the mechanism. Understanding why helps you trust the practice.
The vagus nerve suppresses cortical spreading depression — the slow wave of electrical silence that rolls across the brain surface, triggers aura, and ignites the pain cascade.[7] In animal models, vagus nerve stimulation cut CSD frequency by 40% and slowed its propagation by 15%.[7] It also drives down extracellular glutamate — the brain’s primary excitatory neurotransmitter — in the trigeminal nucleus caudalis, the relay station where migraine pain signals converge.[8]
Then there’s the cholinergic anti-inflammatory pathway. When the vagus fires, it releases acetylcholine. That acetylcholine binds to α7 nicotinic receptors on immune cells and suppresses pro-inflammatory cytokines — TNF-α, IL-6, the molecules that amplify neurogenic inflammation.[9] This matters because migraine involves CGRP and substance P pouring from trigeminal nerve endings, sensitizing pain pathways at their source.[10] Vagal activation doesn’t mask that inflammation. It intervenes in the cascade.
Clinical trials back this up. The PRESTO trial — randomized, double-blind, sham-controlled, 248 episodic migraine patients — showed noninvasive vagus nerve stimulation (nVNS) achieved pain freedom at 30 minutes in 12.7% of patients versus 4.2% for sham, with similar advantages at 60 minutes.[11]
A meta-analysis of six RCTs involving 845 patients found cervical nVNS significantly improved the 50% responder rate (OR 1.64), while auricular nVNS reduced monthly migraine days by 1.8.[12] The PREMIUM II trial reported a 44.87% responder rate for active treatment versus 26.81% sham — with particularly strong results in migraine with aura.[13]
These are FDA-cleared noninvasive vagus nerve stimulation devices. They work.
They also cost roughly $700 per month.[14]
What if you could activate the same nerve — through different doorways — for free?
Technique 1: The Slow Exhale
This is the most studied free vagal activator in existence.
Slow your breathing to roughly 5 to 6 breaths per minute. Extend the exhale longer than the inhale. At this pace, heart rate and breathing synchronize at approximately 0.1 Hz — a frequency researchers call “resonance” — and vagal activity reaches its measurable peak.[15]
The mechanism is elegant. A 2018 review in Frontiers in Human Neuroscience mapped the pathway: slow exhalation activates stretch receptors in the lungs, which send signals up the vagus nerve to the brainstem, which deepens parasympathetic engagement, which further slows breathing.[16] A self-reinforcing loop. Safety signals in, calm signals out.
Does it hold up in practice? A randomized controlled study found that four weeks of daily resonance-frequency breathing — just 20 minutes per session — significantly increased parasympathetic activity and reduced sympathetic dominance.[17] When researchers compared techniques head-to-head, breathing at 6 breaths per minute produced higher HRV than box breathing or the popular 4-7-8 technique.[18]
How to do it
Inhale gently through your nose for 4 seconds. Exhale slowly for 6 seconds. One cycle. Repeat for 5 to 10 minutes. No app. No timer. Just count.
Technique 2: The Cold Face Reset
Splash cold water on your face — forehead, cheeks, the bridge of your nose — and your body executes one of its oldest survival programs.
Temperature receptors in facial skin activate the trigeminal nerve. The trigeminal signals the brainstem. The brainstem fires the vagus. Heart rate drops. Blood redirects to the brain and heart. This is the mammalian diving reflex — the same mechanism that lets seals survive long dives.[19]
A 2023 meta-analysis in Psychophysiology confirmed: the diving response produces moderate to large increases in cardiac vagal activity.[20] A randomized study using the Cold Face Test showed heart rate reduction and lower cortisol during acute stress, with the vagal response kicking in within about 5.6 seconds of cold contact.[21] Water at approximately 10°C triggered the strongest parasympathetic shift.[22]
Five and a half seconds. That’s how fast your nervous system can change direction.
How to do it
Fill a bowl with cool water — around 10 to 15°C (50–59°F) is the sweet spot. You want cold, not ice-cold; the goal is to trigger the dive reflex, not cold shock. Tap water straight from the cold handle usually falls in this range. Hold your breath. Immerse your face for 15 to 30 seconds. Or press a cold, wet cloth against your forehead and cheeks for 30 to 60 seconds. During a prodrome or early attack, this is your fastest reset.
⚠️ When to Seek Emergency Help
A sudden, severe headache unlike anything you’ve experienced — especially with confusion, vision loss, numbness, slurred speech, or stiff neck — demands emergency evaluation. Period. These may signal stroke or another medical emergency, not a typical migraine.
Call your local emergency number immediately. Do not use this article to self-diagnose.
Technique 3: The Hum
This one surprises people. Humming produces mechanical vibrations that travel through your throat, chest, and around your ears — directly stimulating the vagus nerve through its recurrent laryngeal branch and auricular branches.[23]
An fMRI study at the National Institute of Mental Health and Neurosciences examined what happens in the brain during OM chanting. The results: significant deactivation of the amygdala, hippocampus, anterior cingulate, and thalamus — the same limbic structures that quiet down during electrical vagus nerve stimulation for epilepsy and depression. The control condition — making an “ssss” sound — produced none of these effects.[24] The researchers attributed the difference to vibrations reaching the vagal auricular branch near the ear.
The practical data is equally compelling. A Holter-based study found that humming produced RMSSD levels — a gold-standard measure of beat-to-beat vagal activity — comparable to slow-paced breathing and statistically similar to sleep.[23] One extra detail: humming increases nitric oxide output in the sinuses by roughly 15-fold compared to quiet breathing. Nitric oxide dilates blood vessels and modulates neurotransmitter release[23] — a potential bonus for the constriction-prone migraine brain.
How to do it
Inhale through your nose. Exhale while humming on a single low pitch. Feel the vibration in your chest and face. Two to three minutes. You can do this at your desk, in the car, in bed at 3 a.m. with the lights off.
Building Your Vagal Toolkit

Three techniques. Three different doorways — respiratory, thermal, vibratory. One destination: higher vagal tone, lower sympathetic overdrive, a calmer migraine brain.
The key isn’t intensity. It’s consistency. Five minutes of slow breathing each morning. A cold splash after a stressful meeting. A few minutes of humming before bed. Over weeks, daily practice raises your baseline vagal tone — the resting level of parasympathetic activity — rather than just offering momentary relief.[17]
Think of it as physical therapy for your nervous system. One session helps. Twenty sessions change the default.
I’ve lived with migraine for 30 years. I’ve tried medications that cost hundreds of dollars a month, supplements with promising abstracts, devices with blinking lights. The tools I reach for most often cost nothing. A slow exhale takes 10 seconds of attention. A cold splash takes 30. A hum takes one breath.
Your body was designed to respond to these signals. The vagus nerve is waiting. Use it.
⚕️ Important Medical Disclaimer
This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. The author, Rustam Iuldashov, is not a licensed physician, neurologist, or healthcare professional. He is a patient advocate with 30 years of personal experience living with chronic migraine.
All clinical claims in this article are sourced from peer-reviewed research published in indexed medical journals. Study designs and sample sizes are noted where applicable.
Always consult a qualified healthcare provider for questions about your individual health, migraine treatment, or medication decisions.
The vagus nerve techniques described should complement — never replace — prescribed treatments. People with cardiac conditions, particularly bradycardia or heart block, should consult a physician before using cold water immersion techniques. This content was last reviewed for accuracy on March 9, 2026.
References
- Breit S, Kupferberg A, Rogler G, Hasler G. “Vagus Nerve as Modulator of the Brain-Gut Axis in Psychiatric and Inflammatory Disorders.” Frontiers in Psychiatry, 9:44 (2018). doi:10.3389/fpsyt.2018.00044. Study design: Review. n=N/A.
- Waxenbaum JA, Reddy V, Varacallo M. “Anatomy, Autonomic Nervous System.” StatPearls (2024). Study design: Review. n=N/A.
- Koenig J, Williams DP, Kemp AH, Thayer JF. “Vagally mediated heart rate variability in headache patients — a systematic review and meta-analysis.” Cephalalgia, 36(3):265–278 (2016). doi:10.1177/0333102415583989. Study design: Systematic review / Meta-analysis. n=multiple studies pooled.
- Zhang Y, et al. “Heart Rate Variability Analysis in Episodic Migraine: A Cross-Sectional Study.” Frontiers in Neurology, 12:647092 (2021). doi:10.3389/fneur.2021.647092. Study design: Cross-sectional. n=36.
- Chuang CH, Li JY, King JT, et al. “Abnormal heart rate variability and its application in predicting treatment efficacy in patients with chronic migraine.” Cephalalgia, 43(10) (2023). doi:10.1177/03331024231206781. Study design: Prospective cohort. n=chronic migraine patients vs. controls.
- Matei D, et al. “Autonomic imbalance in migraine: decreased SDNN, RMSSD and HF supporting parasympathetic hypofunction.” European Neurology (2015). Study design: Prospective cohort. n=27 migraine + 10 controls.
- Chen SP, et al. (referenced in Yuan et al. meta-analysis). “VNS inhibited CSD frequency by 40% and propagation speed by 15%.” Study design: Preclinical animal model. n=N/A.
- Akerman S, Simon B, Romero-Reyes M. “Vagus nerve stimulation suppresses acute noxious activation of trigeminocervical neurons.” Neurobiology of Disease, 41(1):183–193 (2011). doi:10.1016/j.nbd.2010.08.025. Study design: Preclinical animal model. n=N/A.
- Pavlov VA, Tracey KJ. “The cholinergic anti-inflammatory pathway: a missing link in neuroimmunomodulation.” Molecular Medicine, 9(5-8):125–134 (2003). doi:10.1007/BF03402177. Study design: Review. n=N/A.
- Edvinsson L. “The Trigeminovascular Pathway: Role of CGRP and CGRP Receptors in Migraine.” Headache, 57(Suppl 2):47–55 (2017). doi:10.1111/head.13081. Study design: Review. n=N/A.
- Tassorelli C, Grazzi L, de Tommaso M, et al. “Noninvasive vagus nerve stimulation as acute therapy for migraine: The randomized PRESTO study.” Neurology, 91(4):e364–e373 (2018). doi:10.1212/WNL.0000000000005857. Study design: RCT (double-blind, sham-controlled). n=248.
- Yuan X, et al. “Noninvasive vagus nerve stimulation for migraine: a systematic review and meta-analysis of randomized controlled trials.” Frontiers in Neurology, 14:1190062 (2023). doi:10.3389/fneur.2023.1190062. Study design: Systematic review / Meta-analysis. n=845.
- Diener HC, et al. “Non-invasive vagus nerve stimulation for prevention of migraine: The PREMIUM II trial.” Cephalalgia (2022). doi:10.1177/03331024211063836. Study design: RCT (double-blind, sham-controlled). n=~300.
- American Headache Society (2024). nVNS cost commentary by Dr. Hamilton. americanheadachesociety.org. Study design: Expert commentary. n=N/A.
- Steffen PR, Austin T, DeBarros A, Brown T. “The Impact of Resonance Frequency Breathing on Measures of Heart Rate Variability, Blood Pressure, and Mood.” Frontiers in Public Health, 5:222 (2017). doi:10.3389/fpubh.2017.00222. Study design: RCT. n=3 groups compared.
- Gerritsen RJS, Band GPH. “Breath of Life: The Respiratory Vagal Stimulation Model of Contemplative Activity.” Frontiers in Human Neuroscience, 12:397 (2018). doi:10.3389/fnhum.2018.00397. Study design: Theoretical review. n=N/A.
- Nivethitha L, et al. “Effect of Resonance Breathing on Heart Rate Variability and Cognitive Functions in Young Adults.” Cureus, 14(2):e22187 (2022). doi:10.7759/cureus.22187. Study design: RCT. n=young adults (18–30).
- BYU thesis. “Comparing the Effects of Square, 4-7-8, and 6 Breaths-per-Minute Breathing on HRV, PETCO2, and Mood.” Brigham Young University (2024). Study design: Within-subjects experimental.
- Panneton WM. “The mammalian diving response: an enigmatic reflex to preserve life?” Physiology (Bethesda), 28(5):284–297 (2013). doi:10.1152/physiol.00020.2013. Study design: Review. n=N/A.
- Ackermann S, et al. “The diving response and cardiac vagal activity: A systematic review and meta-analysis.” Psychophysiology, 60(2):e14183 (2023). doi:10.1111/psyp.14183. Study design: Systematic review / Meta-analysis. n=multiple studies.
- Becker S, et al. “Vagus activation by Cold Face Test reduces acute psychosocial stress responses.” Scientific Reports, 12:19270 (2022). doi:10.1038/s41598-022-23222-9. Study design: RCT. n=28.
- “Autonomic Effects of Facial Immersion at Varying Water Temperatures.” European Journal of Cardiovascular Medicine (2025). Study design: Comparative cross-sectional. n=two age groups.
- ScienceInsights (2026). Compiled: Holter-based HRV study during humming; humming vs. slow-paced breathing pilot; sinus nitric oxide measurements. Study designs: various.
- Kalyani BG, Venkatasubramanian G, Arasappa R, et al. “Neurohemodynamic correlates of ‘OM’ chanting: A pilot fMRI study.” International Journal of Yoga, 4(1):3–6 (2011). doi:10.4103/0973-6131.78171. Study design: Pilot fMRI. n=12.

How We Create Content
- Peer-reviewed sources only. Cephalalgia, Neurology, Frontiers in Neurology, Frontiers in Human Neuroscience, Frontiers in Public Health, Psychophysiology, Scientific Reports, Molecular Medicine, International Journal of Yoga, Neurobiology of Disease.
- Study transparency. Study design and sample sizes noted for all clinical references.
- Source verification. All claims backed by numbered references with DOI links.
- Experience + Science. 30 years personal migraine experience combined with peer-reviewed evidence.
- Regular updates. Articles reviewed when significant new research emerges.
- No conflicts of interest. No funding from neuromodulation device manufacturers, pharmaceutical firms, or wellness product companies.
Your Nervous System Deserves a Diary.
Migraine Companion helps you track attacks, log self-care practices like breathing and vagal exercises, and discover which habits actually move the needle on your migraine pattern.
Last reviewed: March 2026
Next scheduled review: September 2026